Peer Review Articles About the Genetic Cause of Autism
Abstruse
Background
Autism is all the same considered a very complex disease, since it has diverse etiology, with multiple factors plainly associated with its appearance. Nevertheless, none of them reveals to be totally responsible for its development.
Nowadays, this disorder is considered to take a strong genetic component with the interaction of several genes. Furthermore, other diseases with well-known etiology might also be related with autism.
Methods
The aim of this review is to discuss, through bibliographic search, genetic factors involved in autism evolution.
Results
Some of the candidate genes of idiopathic autism (90-95% of all cases) related to brain metabolism are AVPR1a, DISC1, DYX1C1, ITGB3, SLC6A4, RELN, RPL10 and SHANK3.
Conclusion
All these genes are responsible for symptoms that tin can explain the origin of this status. Autism is a multifactorial disorder in which genetic and environmental factors interact, triggering its development.
Keywords
Autism spectrum disturbances, Genes determining autism, Idiopathic autism
Introduction
Since the beginning of human being existence, communities exclude or fail those that deviate from normal standards at physical or mental levels. A lot comes from the unfounded myths and believes and from the unknown itself. Nowadays, interest on this population is increasing and consequently enquiry is focusing on deepening knowledge on these disturbances aiming their integration on a society build apart from those who have special needs.
The word "autism" comes from "autos", greek give-and-take that ways "itself" or "to itself". It is a syndrome with extremely variable phenotype, being considered a disturbance of human development.
Reports on the increase in autism prevalence in the population, studies apropos treatment efficacy and high costs in teaching and intendance of these patients has fabricated this pathology a focus of great interest in public health.
It is estimated that the prevalence of Disturbances of Autism Spectrum (DASs) is 0.5-1% and seems to increase fifteen% each year. The discussion between a real increase of these disorders or a possible improvement in diagnosis, remains [1].
Autism Spectrum
History and definition
The study of autism started 7 decades ago. It was described for the get-go fourth dimension in 1943 by the Austrian medico Leo Kanner, in his scientific paper "Autism Disturbances of Melancholia Contact" [two]. In this work, the writer started to group a set of apparently characteristic behaviours, present in eleven children followed past him, mainly boys. In theory, these behaviours could assistance to identify children with this disturbance, that showed perceived, emotional and cognitive arrears [ii-4]. In the 2 following decades and despite the publication of that study, there was a lack of interest on this disorder.
However, kickoff results pointed to the similarity between the terms Autism and Kid Schizophrenia, that probably led to their incorrect differentiation. Confirming this fact, the concept of autism had already been introduced by Bleuler in 1911, by referring to schizophrenia as a limitation in homo relationships and the outside globe [5]. In 1971, the two concepts were finally dissociated due to differences in symptoms (such as the age of onset of outset symptoms), family history and differences in response to handling of adults suspected to have schizophrenia/child autism [ane].
After Kanner, Hans Asperger [6] published a paper entitled "Childhood Autistic Psychopathology", based on the report of four children described equally carriers of the same resistance in the establishment of social contact, and the same pattern of restrict interests, only having sophisticated language skills [6]. At this moment, the term Asperger Disturbance appeared [four,7]. Nowadays, it is hands distinguished from archetype autism [8].
Afterward the work of these 2 scientists, other clinical studies followed up, however, just with the publication of the 4th edition of the Diagnostic and Statistical manual of Mental Disturbances (DSM-Iv), of the American Association of Psychiatry, autism was classified equally a blazon of Global Disturbance of Development (GDD) [iv,9]. Nowadays, information technology is described as a alter in normal development of a child that shows abnormal "advice, socialization and restrict and stereotyped behaviours" [iv]. Among GDDs, information technology is possible to distinguish unlike types: Asperger syndrome; Global Disturbance of non-specified Development (GDD-NS); Rett Syndrome and Kid Disintegrative Disturbance [iv,5,9], (Table 1).
Table i: Diagnosed types of GDDs co-ordinate to the classification of DSM-Iv-TR [5]. View Tabular array 1
According with Lorna Wing, the caste of autism varies with the deficits observed over time at social interaction, exact and non-verbal communication and the use of imagination, being called the "Triade of Social Impediments" [x]. Deviations of these disturbances result from their very heterogeneous and by and large unknown aetiology [11]. So, clarification of autistic spectrum goes far from strict definitions, including individuals with low cerebral potential that reveal deficit on reciprocal verbal advice and repetitive behaviours together with mental retardation and those having loftier cognitive potential that fifty-fifty having arrears in social interaction with repetitive and stereotyped behaviours, practise not show retardation in speech development (similar in the Asperger syndrome) [iv].
GDDs (amid them are ASDs) involve a group of clinical changes with early onset where various bones areas of behaviour and development are simultaneously compromised. Rett syndrome and Disintegrative Disturbance of Second Childhood are too included in this group [v,12].
Behaviour analysis of ASDs
Although now a days noesis concerning autism is much more than prefound, it all the same surprises due to the diversity of characteristics that patients can show.
Unremarkably, the autistic child has normal physical [iii,xiii]. However, these children too show an irregular profile of evolution that is detectable in the first 3 years of life, being present till adulthood. The Triade of Social Impediments is characterized past a strict and continuous design with intelligence levels varying from mental retardation to an extraordinary operation in certain cognitive domains (similar music, arts, mathematic, retentiveness) or savant capacities [3,4,10,14]. Although 80% of autistic children show mental retardation, savant capacities can exist, however the global intelligence ratio is low [3,12,14]. The difference between mental retardation and autism should exist pointed out: The first one shows a uniform evolution arrears; while the concluding presents an irregular profile, with differentiated degrees of commitment.
The post-obit classification and diagnosis systems allow to distinguish autism from other disorders: International classification of Diseases of the World Wellness Organization and the Manual of Diagnosis and Statistics of Mental Disorders from the American Academy of Psychiatry (DSM-4). In these systems the term Child Autism was replaced by Autistic Disturbance, officially separating it from Asperger syndrome [xv].
According with Siegel [8] echolalia (child repeats the aforementioned sound consecutively), incapacity to play symbolic games, prenominal inversion (utilise of the tertiary person instead of the beginning), abnormal voice sound, absence or deficit of speech communication, peculiar relation within animate objects, stereotyped interests, repetitive behaviours, deficit in social, emotional and interests share and trouble in establishing visual and physical contact are common characteristics of autism [8]. Other symptoms ofttimes observed in these individuals are hyperactivity, attending deficit, impulsivity, aggressivity and self-aggressivity [thirteen].
Individuals with Asperger disturbance reveal social deficits and restricted interests. However, their speech capacities remain intact, or show speech capacities above boilerplate for their historic period [4,viii].
Individuals with Global Disturbance of non-specified Development show changes in one or more than developmental areas, even so, these are not enough to exist included in the autistic or Asperger disturbances, since they are lower in number or intensity [xvi].
The phenotypic heterogeneity or high variability observed in behavioural standards and in social and advice capacity gave rise to the predominant use of the term Autistic Spectrum Disturbances [15].
The stardom between autistic disturbance and the remaining ASDs is more than complicated due to the simultaneous occurrence of one or more psychiatric and neurological disorders in most patients (72%), including: Attention/hyperactivity deficit, tic disorder, dyspraxia (neurological motor dysfunction), dyslexia (reading, writing and spelling difficulty), obsessive-compulsive disorder, phobias, feet, humor, slumber and feeding disturbances [17].
Prevalence
In the Portuguese population, the prevalence of DASs is one in a thousand children [3,17]. It is estimated that 60-seventy in 10,000 individuals endure from a Global Disturbance of Development, and 20 in each 10,000 are disturbances of the autistic spectrum (one third being Asperger disturbance). These values make DASs the most frequent forms of child developmental disturbances, and a ascension is existence observed over the terminal decades [18]. However, prevalence differs between gender, being four times higher in men. All the same, an autistic female is usually more than afflicted at cerebral level [3,17].
Aetiology
Since Kanner studies, some feature aspects of autism started to be analysed in the personality of parents and affected children. Initially, the crusade of autism was associated with parents emotionally and socially cold. Later, scientific studies associated autism to mental retardation, genetic syndromes, epilepsy and other neurological weather that had the organic bases of autism and related disorders [5]. These take strongly contributed to elucidate the biological aspects of ASDs and demonstrated that these are complex conditions, with multiple aetiologies and diverse degrees of severity. Although evidences demonstrate that most cases of ASDs consequence from genetic causes, the expression of those genes can be modulated by environmental factors from the gestational flow. It should be emphasized that several deficiencies with cerebral interest associated with ASDs, occur during the first and second trimester of pregnancy (teratogenic issue) [one].
Although a large written report using microarray tests performed by Shen, et al. [19] observed that 80% of analysed autistic children had a normal genome, several other studies indicate for the existence of a narrow correlation betwixt genetic predisposition (in a higher place 90%) and environmental factors [4]. Some consistent changes during gestation of affected individuals are known, nonetheless, pre-natal diagnosis is still not possible, mainly because no concrete traits can exist identified. The starting time alert sign is the deficient social interaction of the child, mainly observed betwixt 6 months and 3 years of age [15].
In autism aetiology, "it is observed a drastic decrease in take a chance for family members of the second or third degree, pointing to the involvement of multiple interactive genes", that influence each other [twenty]. Notwithstanding, although numerous investigations at the pharmacological, pathological, electrophysiological and imaging levels take been done, ASDs aetiology is still under give-and-take [21].
Diagnosis
Since information technology is all the same not possible the use of genetic markers for this disorder, diagnosis is commonly based on meticulous investigation of the history of the patient and family inquiry (cognitive and behaviour capacities) according with Autism Diagnostic Interview-Revised (ADI-R) and the Autism Diagnostic Ascertainment Schedule (ADOS) [16].
Information technology is believed that autism appearance is related with some brain anomaly, non yet defined, associated with a genetic cause. Since ASDs show a very heterogenous aetiology, no definitive medical examination or cure for this type of disorders has been adult yet. For this reason, only in very few cases definitive diagnosis happens before xx-iv months of historic period (a well established diagnosis is ordinarily done between 3 and 6 years of historic period) [22].
In this manner, evaluation should exist done by i or more professionals with medical background and several years of clinical experience. The doctor tries to investigate, through several exams, the beingness of disorders with known causes that tin atomic number 82 to a child autistic picture, such equally the Ten-fragile syndrome or the Rett disturbance [15].
Clinical genetic tests can as well be performed, and the commonly used strategy involves, in the offset place, a chromosome microarray analysis that allows the detection of chromosome copy number variation as well every bit the being of chromosomal deletions or duplications of considerable size. The 2nd approach involves molecular Deoxyribonucleic acid tests for specific genes or even whole genome sequencing. For instance, patients can exist tested for Frail Ten syndrome by the analysis of specific unmarried cistron or, in the presence of a specific characteristic/condition, search for a set of genes that have been associated with those characteristics.
Autism genesis is divided in Secondary Autism (with environmental agents, chromosomal anomalies or identified genetic changes) and in Idiopathic (without known cause and involving more than than x genes), being this last ane the about common [3].
Secondary Autism: Genetic Factors
Several genetic diseases are related with an increased risk of ASDs, being responsible for 5-10% of total diagnosed cases. Since autism prevalence is higher in men, several studies have proposed that the genetic influence of the X chromosome increases the susceptibility for ASDs [14].
X-Fragile syndrome (XFS)
Patients usually testify developmental problems, mainly speech and motor retardation, or even, autistic behaviours. Since the locus of the main involved cistron is the X chromosome (Xq27.3), the probability of X-frail syndrome development is increased in males. In nigh cases (99%), the disease is related with the loss of role of the FMR1 gene, that results from the presence of multiple copies of the triplet repeat CGG in the 5' untranslated region (5' UTR) of that gene. The FMR1 protein (FMR1P - fragile Ten mental retardation ane poly peptide) is the product of the FMR1 cistron, and is mainly present in neuron cytoplasm, existence involved in of import processes like ribosomal translation and maturation of synapse structure and function, having a suppressor consequence at the post-synaptic region [14,23].
The number of CGG repeats is variable and tin can be classified as a pre-mutation (59-200 repetitions) or full mutation (to a higher place 200 repeats). In the presence of a pre-mutation transmitted by the mother, the meiotic instability might result in a complete mutation [14].
Autism has a high prevalence in XFS individuals, reaching 25-33%. The FMR1 protein tin touch the expression of several genes involved in autism development. However, XFS is distinguishable from autism by the presence of a specific biomarker, the aberrant expansion of the CGG repeat in the Ten chromosome [14,23].
Down and Pradel-Willi/Angelman syndrome
Downwardly syndrome is the well-nigh frequent cytogenetic bibelot in patients with ASDs (7-10% of individuals are carriers of ASDs), followed by the one found in the region 15q11-xiii (present in 1-iv% of autistic patients). When the 15q11-13 region suffers duplication or inversion, a high incidence of epilepsy in childhood is observed, besides as muscular hypotony and motor coordination problems, together with strong or moderate mental retardation, absence or delayed speech and astringent hyperactivity. If deletions occur in the referred chromosomic regions, maternal or paternal, imprinting diseases will develop: Angelman and Prader-Willi syndromes respectively [24].
Rett syndrome
Rett syndrome associated with the MeCP2 cistron, is a dominant disease associated with the X chromosome, being considered 1 of the factors responsible for a modest number of autism cases. This syndrome is commonly lethal in boys. The most frequent mutations occur in exons 2, 3 and four of the mentioned factor [14].
Epilepsy
Some researchers refer that epilepsy episodes in individuals diagnosed with ASDs, occur in a casual course. Data prove an increased chance of epilepsy in ASDs individuals, resulting from a Fundamental Nervous Organisation bibelot characterized by neuropathological changes. One tertiary of autistic individuals develop epilepsy, since dysfunctions in the CNS strongly increase the adventure of developing it. The prevalence of autistic children with epilepsy varies betwixt 5 and 46% [13,21].
Schizophrenia
This condition can be associated with exposure to infections before birth and subsequent inflammatory response. In the aforementioned mode, autism tin can result from this phenomenon since it shares with schizophrenia several encephalon morphological changes [one].
According with Meyer et al. [1] infections in women during the critical periods of pregnancy tin can pb to astute inflammation associated with the presence of cytokinin in the foetal system, especially at brain level. This affects negatively neuronal evolution processes: Proliferation, migration and jail cell survival. In this way, astute inflammation during foetal neuronal evolution tin can pb to the formation of aberrant neuronal substrates that interfere with social, cognitive and emotional behaviour processes, amidst others.
Mental retardation
The AGTR2 factor, present in the X chromosome (Xq22-q23), seems to be involved in the development of mental retardation in autistic individuals, since these patients show deletion of this cistron. However, the Xq13-q21 region that contains genes of the neuroligins family is fifty-fifty more important in the evolution of this condition. Neuroligins are crucial in processes of cellular interaction, through adhesion molecules, betwixt neuronal cells [24,25].
Approximately 75-80% of autistic children suffer a severe mental retardation [5].
Idiopathic Autism
Idiopathic autism is the blazon of autism with unknown aetiology, representing 90-95% of full diagnosed cases. Several genes have been tested every bit possible candidates for its development, and, so far, more than than 10 genes have been identified [5,11].
Genetic Bases of Autism
Several psychiatric diseases have strong evidences of genetic involvement in their origin, and among them are schizophrenia, bipolar disturbance and autism. In 1977, a written report with mono and dizygotic twins described for the first time the genetic predisposition of autism [26,27].
Nowadays, population studies suggest that the model that better describes DASs is multifactorial [13,20,28,29] with a cyclopedia of sixty-92% in monozygotic twins and 0-10% in dizygotic twins [thirty]. Differences found in studies between monozygotic twins support the multifactorial model, demonstrating the importance of environmental factors.
Several studies were performed to clarify genetic factors associated with the disease. Autism symptoms that suggest a potent genetic component are convulsions, mental deficiency, neurons and synapse subtract in amygdala, hippocampus and cerebellum, increased size of encephalon, and increased level of circulating serotonin. Even studies with monozygotic twins evidence a significant concordance, as opposed to dizygotic twins. Non-twin siblings present a risk of developing autism ranging from 0-30%, and this risk is much higher than in the general population [31].
The comparing of the mentioned populational groups, likewise every bit the difference between men and women, shows epistatic effects (hierarchy between alleles) that involve an interaction between several genes, suggesting the function of ecology factors [32].
Genes Involved in Autism: Candidate Genes
Studies on monozygotic and dizygotic twins, adopted children and their families helped the institution of a stiff genetic component in autism. Still, analysis performed on the genome of autists failed in the establishment of consistent signs of linkage. None of cognitive and affective diseases, as well equally certain psychoses, follow a heritage design according with Mendel's laws, reinforcing the hypothesis of the involvement of multiple genes [24].
Since it is a circuitous disorder with the involvement of several variants, each contributing with a reduced chance to phenotype, the identification of susceptibility genes has been difficult. Moreover, hypotheses that back up the presence of synergism and/or epistas is between multiple candidate genes are based on chromosomic changes that are not always enough for affliction development [24]. So, traditional methods of linkage used in almost studies, are insufficient to detect modest genetic furnishings, in typically small samples. It is then necessary to select candidate genes based on the type of coded proteins that play an of import function in autism development [33].
A big number of involved chromosomes endure translocations and inversions. These changes result in interruption of genes likewise every bit deletions and duplications that are responsible for differences in gene expression. The near frequently reported mutations are duplications in 15q11-q13 and deletions in 2q37, although nigh of them are undetectable by karyotype assay [34].
According with Freitag [27] some chromosomic deletions in 2q37, 7q31, 22q11 and 22q13.3, are also important in the cytogenetic evaluation of autism. Chromosomic micro deletions responsible for certain syndromes, are associated with the appearance of secondary autism: Velocardiofacial syndrome, DiGeorge syndrome and Facial Conotruncal bibelot syndrome.
Several genes have been associated with the development of autism. Withal, the appearance of this condition seems to involve the combination of changes in several genes, behaving in an additive manner.
In this study, encephalon-related genes though to take a function on the prevalence of this disorder are described (Figure 1). Nonetheless, many other genes seem to play a role in the development of this status, as is the case of genes encoding ion-channels.
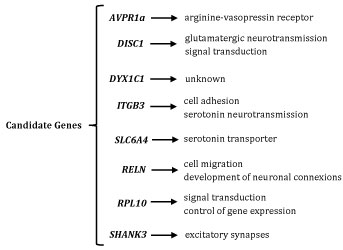 Figure 1: Brain-related genes though to have a office on the prevalence of Autism. View Figure 1
Figure 1: Brain-related genes though to have a office on the prevalence of Autism. View Figure 1
AVPR1a factor
This factor is located at the long arm of chromosome 12 and encodes the arginine-vasopressin receptor (AVPR). Mutations in this gene lead to changes in the number of these receptors. The outset report on changes in this factor associated with ASDs dates from 2002. In this study, researchers genotyped two microsatellite polymorphisms from the 5' flanking region of the AVPR1a gene. This work establish significant transmission disequilibrium between autism and ane of the microsatellite markers. Moreover, ten single nucleotide polymorphisms were identified by screening two kb of the 5' and coding region of the gene [35].
The CNS shows differences in receptor distribution that might interfere with the effects of the AVP system, among which are: Vocal position; sexual and parental behaviour; aggressivity; and social recognition. The AVP organization reveals stronger effects in males [28].
According with Wassink et al. [28] autism susceptibility tin can increase by changes in the cistron coding for the receptor 1a of the AVP system (AVPR1a). These changes lead to deficient social interaction, lack of parental behaviour, severe aggressivity, among other symptoms.
DISC1 gene
This gene is present in the locus 1q42 that contains the TRAX and DISC2 genes (involved in the regulation of DISC1 gene expression). The DISC1 gene codes for a protein with an essential part in growth and neuronal migration, in synaptogenesis, in glutamatergic neurotransmission (whose molecular processes of synaptic modification are among the nigh common in all CNS), and in cAMP signal transduction [29].
Kilpinen, et al. [29] were able to constitute an association betwixt autism and a DISC1 intragenic microsatellite (D1S2709). A single nucleotide polymorphism in the DISC1 gene (rs1322784) was too associated with male patients having ASDs [29].
The discovery of interaction betwixt the TRAX and DISC2 genes and the DISC1 cistron raised a new hypothesis that is based on the possibility of molecular mechanisms leading to brain dysfunctions at the affective and cognitive levels.
DYX1C1 gene
It is present in locus 15q21 and codes for a protein whose function is withal not completely understood. However, it has already been established that it is expressed in a subgroup of human being neuronal and glial cells, existence the beginning candidate gene for dyslexia and the 2nd associated with language disturbances. In the presence of genetic change, like a translocation, the factor is interrupted and can lead to two variants. One of these is related with the loss of attachment place to several linking factors. The 2nd leads to the appearance of a premature stop codon and consequent loss of four amino acids at the finish of the coded protein [25].
Dyslexia is a disturbance characterized by problems in learning to read or write (contained of the intelligence degree, social extract or interests of the private). This phenotype has some interest in the study of ASDs since it might represent other disturbances with linguistic communication evolution delay. Withal, information technology doesn't seem likely to be a very relevant factor in autism development [25].
ITGB3 gene
Information technology is located in chromosome 17 (q21.three) and codes for β-integrin iii. This poly peptide is nowadays in jail cell surface, especially in platelets. Integrins are known past their participation in cell adhesion and in metabolism and neurotransmission of serotonin (5-HT). Integrin receptors accept shown an important role in signalling, being able to influence transcription and translation [30,36].
According with Napolioni et al. [xxx] the presence of a single nucleotide polymorphism located at the 5' terminal of theITGB3 factor, is strongly related with loftier plasma levels of 5-HT, ane of the characteristics most oft establish in autists (around thirty% of autistic individuals) [36,37]. Allelic variants of theITGB3gene were identified in some studies, both isolated or interacting with allelic variants of the gene coding for v-HT transporter (SLC6A4 gene, located close to the ITGB3 gene) [thirty,36].
Moreover, Schuch, et al. [38] analysed v single nucleotide polymorphisms in the ITGB3 gene. These researchers observed small clan of the rs15908 and rs12603582 polymorphisms with symptoms of echolalia, epilepsy and aggressivity, characteristics of ASDs [38].
Genes that influence the serotonin organisation are strong susceptibility genes, since selective drugs for the serotonin organisation reveal more efficacy in the treatment of some misbehaviour establish in autism (similar disturbances related with anxiety and aggression) [36].
SLC6A4 gene
This gene is in the long arm of chromosome 17 and codes for the serotonin transporter. This is a chemical substance that acts at encephalon level, through signal transmission between neurons (synapses). The part of serotonin system in autism is not totally antiseptic nonetheless, however, it is known that polymorphisms of this gene tin modulate the recapture of the transporter, explaining the occurrence of hyper-serotonin in some autistic individuals [36,39].
According with Longo [5] insertion/deletion polymorphisms located at the promoter of the SLC6A4 gene accept been identified. Serotonin levels in synapses are regulated by its transporter and, when this one becomes active, serotonin builds-up in blood platelets instead of ascension in synapses (where information technology is low). This can lead to of import behaviour changes that determine the advent of autism [5,36].
Adamsen et al. [40] identified iii heterozygous mutations in the SLC29A4 gene: c.86A > Thousand (p.Asp29Gly) in two patients, c.412G > A (p.Ala138Thr) in 5 patients and c.978 T > 1000 (p.Asp326Glu) in 1 patient. Expression of mutations p.Ala138Thr and p.Asp326Glu in cells revealed pregnant reduced send uptake of serotonin and dopamine, linking these mutations to ASD although with depression brain serotonin. Dysfunction of this protein is speculated to raise serotonin prenatally, exerting a negative feedback inhibition through serotonin receptors on development of serotonin networks and local serotonin synthesis [40].
RELN gene
This gene is present in locus 7q22 and codes for a protein with an important role in migration of various jail cell types and in the evolution of neuronal connexions. Information technology is believed that the RELN gene can affect the evolution of autism [33].
According with Skaar et al. [33] one of the about important furnishings of the deletion of this gene in rats, is the abnormal formation of cerebral cortex. Moreover, the study of this gene revealed its importance in the correct germination of brain structures due to the orientation that they confer in migration of neuronal precursors. According with these data, the RELN cistron is related with several neurogenetic diseases (like schizophrenia and bipolar disorder), that show low levels of mRNA and RELN protein in multiple encephalon areas. The following genetic changes tin can be pointed out: Expansion of a trinucleotide polymorphic repeat (GGC) and haplotypes with replacement of two bases of 1 exon [24,33].
Moreover, Tian [41] identified two mutations in the RELN gene, and the grand.504742G > A polymorphism, nowadays in exon60, showed a pregnant clan with autism in a Chinese Han population.
Some studies reveal linkage picks in the long arm of chromosome 7 that contains the RELN gene, and other susceptibility genes for autism, namely in the region 7q22-q33 [24,33]. Attending should be given to this cistron, since changes observed in cerebellar neurons have impact in autism development [24].
RPL10 gene
It is present in chromosome Xq28 and codes for a family of ribosomal L10 proteins, that participate in the control of cistron expression and are probably involved in cell signalling pathways. Mutations in the RPL10 factor (involving amino acrid replacement) allow translation but a premature stop of protein synthesis occurs [42].
There is a marked difference in autism prevalence betwixt males and females, being men the most frequently affected, suggesting a possible involvement of the X chromosome. The beingness of linkage with markers in Xq22.3, Xq13-q26 and Xq27-q28 has been demonstrated. Changes in genes present in the region Xq28 lead to predisposal to mental retardation, that is oftentimes associated with autism [42].
Klauck et al. [42] accept identified two missense mutations in the RPL10 gene in two contained families with autism. These mutations are the amino-acid substitutions L206M and H213Q at the C-last end of RPL10 protein that leads to changes in the regulation of the translation process. These researchers suggested as a model for the development of autistic disorder, that a change in translational part has impact on cerebral functions mediated through the limbic system [42].
SHANK3 factor
Information technology is nowadays in chromosome 22 (q13.3) and codes for a poly peptide (expressed at cortex, hippo campus and cerebellum levels) involved in excitatory synapses in front of the pre-synaptic active zone, and in the formation of intracellular protein complexes, past the establishment of connexions that favour protein interactions [43].
Several studies refer the identification of duplications in the SHANK3 factor that seem to have an important part in autism [43]. Cases of deletion of 22q13.iii with interruption or removal of the SHANK3 gene accept been described. The resultant phenotype includes delay in expressive linguistic communication, severe mental retardation and autism [43].
A single nucleotide polymorphism (rs9616915) is a T > C change in exon half dozen, that leads to a substitution of isoleucine to threonine and directly affects SHANK3 gene office. Mashavekhi et al. [44] were able to associate this mutation to increased risk of autism development.
Conclusion
Several advances in the written report of autism genetics accept been washed, leading to drastic changes in the concept of autism, in the last decades.
According with the complexity of disturbances of the autistic spectrum, the analysis of isolated genes is not conclusive. It is very unlikely that whatsoever study performed with a candidate cistron, covers a high percentage of sample population, consequently its inclusion in phenotype is difficult to identify.
Nowadays, nearly genetic studies focus on specific regions of chromosomes according with the probability of the corresponding genes being related with the observed characteristics of the affliction. Obtained knowledge on genetic or environmental factors is very important for correct diagnosis and treatment and may allow prevention of the disorder.
A lot is still to be clarified in the autism spectrum disturbances, since information technology is likely that several susceptibility factors are involved and some all the same to be discovered. It is urgent to identify genetic variants not even so detected by the conventional genotyping studies, focusing on simultaneous analysis of multiple loci.
Diagnosis criteria used for autistic spectrum disturbances, accept been improved. The ideal diagnosis would be the identification of genetic variants responsible for specific autistic phenotypes.
It is undeniable the contribution of heritance in autism disease but without considering ecology factors, information technology becomes bereft to explicate this complex affliction.
Contribution of Authors
Authors have equally contributed to the elaboration of this paper.
Compliance with Ethical Standards
No funding was used in this study.
Conflicts of Interest
Authors declare that there are no conflicts of interest.
Ethical Approval
This article does not incorporate any studies with homo participants or animals performed by whatever of the authors.
References
- Meyer U, Feldon J, Dammann O (2011) Schizophrenia and autism: Both shared and disorder-specific pathogenesis via perinatal inflammation? Pediatr Res 69: 26-33.
- Kanner L (1943) Autistic disturbances of affective contact. The Nervous Child 2: 217-250.
- Folstein SE, Rosen-Sheidley B (2001) Genetics of autism: Complex aetiology for a heterogeneous disorder. Nat Rev Genet 2: 943-955.
- Gonçalves AA (2011) Dissertação: Os Modelos de Intervenção são eficazes para melhorar a inclusão de crianças com Autismo. Escola Superior de Educação Almeida Garrett. Lisboa.
- Longo D (2009) Influência de fatores genéticos ambientais nos transtornos do espectro autista. Universidade Federal practice Rio Grande do Sul.
- Asperger H (1944) Die "Autistischen Psychopathen" imkindesalter. Archivfür Psychiatrie und Nervenkrankheiten 117: 76-136.
- Johnson CP, Myers SM, the council on children with disabilities (2007) Identification and evaluation of children with autism spectrum disorders. Pediatrics 120: 1183-1215.
- Siegel B (2008) O mundo da criança com autismo. Compreender e tratar perturbações practise espectro practice autismo. Porto Editora, Porto.
- Hughes Five (2012) Epidemiology: Complex disorder. Nature 491: S2-S3.
- Happé F, Ronald A, Plomin R (2006) Time to give up on a single explanation for autism. Nat Neurosci 9: 1218-1220.
- Ecker C, Spooren Westward, White potato DG (2013) Translational approaches to the biological science of Autism: Faux dawn or a new era? Mol Psychiatry xviii: 435-442.
- Fly L (1997) The autistic spectrum. Lancet 350: 1761-1766.
- Veenstra-Vanderweele J, Blakely RD (2012) Networking in autism: Leveraging genetic, biomarker and model organization findings in the search for new treatments. Neuropsychopharmacol 37: 196-212.
- Santos PAC (2010) Análise de Mutações nos genes FMR1 e MTHFR em pacientes com transtornos exercise espetro autista idiopático. Universidade Federal exercise Rio Grande do Sul.
- Oliveira Chiliad (2009) Autismo: Diagnóstico e Orientação. Parte I - Vigilância, Rastreio eastward Orientação nos cuidados primários de saúde. Acta Pediatr Port twoscore: 278-287.
- Oliveira G, Ataíde A, Marques C, Miguel T, Coutinho AM, et al. (2007) Epidemiology of autism spectrum disorder in Portugal: Prevalence, clinical characterization and medical conditions. Dev Med Child Neurol 49: 726-733.
- Oliveira G, Diogo L, Grazina Grand, Garcia P, Ataíde A, et al. (2005) Mitochondrial dysfunction in autism spectrum disorders: A population-based study. Dev Med Child Neurol 47: 185-189.
- Fombonne E (2009) Epidemiology of pervasive developmental disorders. Pediatr Res 65: 591-598.
- Shen Y, Dies KA, Holm IA, Bridgemohan C, Sobeih MM, et al. (2010) Clinical genetic testing for patients with autism spectrum disorders. Pediatrics 125: E727-E735.
- Correia C (2008) Epidemiologia Genética. RevFactores de Risco 8: 60-65.
- Spence SJ, Shneider MT (2009) The part of epilepsy and epilepti grade EEGs in autism spectrum disorders. Pediatr Res 65: 599-606.
- Landa RJ (2008) Diagnosis of autism spectrum disorders in the starting time 3 years of life. Nat Clin Pract Neurol four: 138-147.
- Belmonte MK, Bourgeron T (2006) Fragile X syndrome and autism at the intersection of genetic and neural networks. Nat Neurosci 9: 1221-1225.
- Carvalheira G, Vergani N, Brunoni D (2004) Genética do Autismo. Rev Bras Psiquiatr 26: 270-272.
- Ylisaukko-Oja T, Rehnström Chiliad, Auranen One thousand, Vanhala R, Alen R, et al. (2005) Analysis of four neuroligin genes every bit candidates for autism. Eur J Hum Genet 13: 1285-1292.
- βlvarez I, Camacho-Approach I (2010) Bases genéticas del Autismo. Artículo de revision. Acta Pediatr Mex 31: 22-28.
- Freitag CM (2007) The genetics of autistic disorders and its clinical relevance: A review of the literature. Mol Psychiatry 12: two-22.
- Wassink TH, Piven J, Vieland VJ, Pietila J, Goedken RJ, et al. (2004) Examination of AVPR1a equally an autism susceptibility gene. Mol Psychiatry nine: 968-972.
- Kilpinen H, Ylisaukko-Oja T, Hennah W, Palo OM, Varilo T, et al. (2008) Association of DISC1 with autism and Asperger Syndrome. Mol Psychiatry xiii: 187-196.
- Napolioni 5, Lombardi F, Sacco R, Curatolo P, Manzi B, et al. (2011) Family-based association study of ITGB3 in autism spectrum disorder and its endophenotypes. Eur J Hum Genet 19: 353-359.
- Mendelsohn NJ, Schaefer GB (2008) Genetic evaluation of autism. Semin Pediatr Neurol 15: 27-31.
- Dawson G, Estes A, Munson J, Schellenberg Yard, Bernier R, et al. (2007) Quantitative cess of autism symptom-related traits in probands and parents: Broader Phenotype Autism Symptom Scale. J Autism Dev Disord 37: 523-536.
- Skaar DA, Shao Y, Haines JL, Stenger JE, Jaworski J, et al. (2005) Analysis of RELN gene as a genetic take chances factor for autism. Mol Psychiatry 10: 563-571.
- Castermans D, Vermeesch JR, Fryns JP, Steyaert JG, Van de Ven WJ, et al. (2007) Identification and characterization of the TRIP8 and REEP3 genes on chromosome 10q21.3 every bit novel candidate genes for autism. Eur J Hum Genet 15: 422-431.
- Kim SJ, Immature LJ, Gonen D, Veenstra-VanderWeele J, Courchesne R, et al. (2002) Transmission disequilibrium testing of arginine vasopressin receptor 1A (AVPR1A) polymorphismsin autism. Molecular Psychiatry 7: 503-507.
- Weiss LA, Kosova G, Delahanty RJ, Jiang Fifty, Melt EH, et al. (2006) Variation in ITGB3 is associated with whole-claret serotonin level and autism susceptibility. Eur J Hum Genet xiv: 923-931.
- Cantankerous South, Kim SJ, Weiss LA, Delahanty RJ, Sutcliffe JS, et al. (2008) Molecular genetics of the platelet serotonin system in kickoff-caste relatives of patients with autism. Neuropsycopharmacol 33: 353-360.
- Schuch JB, Muller D, Endres RG, Bosa CA, Longo D, et al. (2014) The role of β3 integrin cistron variants in autism spectrum disorders-diagnosis and symptomatology. Cistron 553: 24-30.
- Coutinho AM, Oliveira G, Morgadinho T, Fesel C, Macedo TR, et al. (2004) Variants of the serotonin transporter cistron (SLC6A4) significantly contribute to hyperserotonemia in autism. Mol Psychiatry nine: 264-271.
- Adamsen D, Ramaekers V, Ho HT, Britschgi C, Rüfenacht V, et al. (2014) Autism spectrum disorder associated with low serotonin in CSF and mutations in the SLC29A4 plasma membrane monoamine transporter (PMAT) factor. Mol Autism 5: 43.
- Tian P (2012) RELN cistron polymorphisms and susceptibility to autism in Chinese Han population. Neurol India 60: 581-584.
- Klauck SM, Felder B, Kolb-Kokocinski A, Schuster C, Chiocchetti A, et al. (2006) Mutations in the ribosomal protein gene RPL10 suggest a novel modulating affliction mechanism for autism. Mol Psychiatry 11: 1073-1084.
- Sykes NH, Toma C, Wilson N, Volpi EV, Sousa I, et al. (2009) Copy number variation and association assay of SHANK3 as a candidate factor for autism in the IMGSAC collection. Eur J Hum Genet 17: 1347-1353.
- Mashavekhi F, Mizban Due north, Bidabadi East, Salehi Z (2016) The clan of SHANK3 cistron polymorphism and autism. Minerva Pediatr.
Commendation
Source: https://clinmedjournals.org/articles/iacod/international-archives-of-communication-disorder-iacod-2-011.php?jid=iacod
0 Response to "Peer Review Articles About the Genetic Cause of Autism"
Post a Comment